Boswellia serrata — Indian Frankincense
Boswellia Serrata
Boswellia Serrata
(Frankincense)
Extract
Research-based guidance on Boswellia serrata and standardized frankincense extracts — including composition, studied health benefits, safety considerations, traditional use, and current clinical evidence.
Educational only; not medical advice. Summarises research findings and limitations.
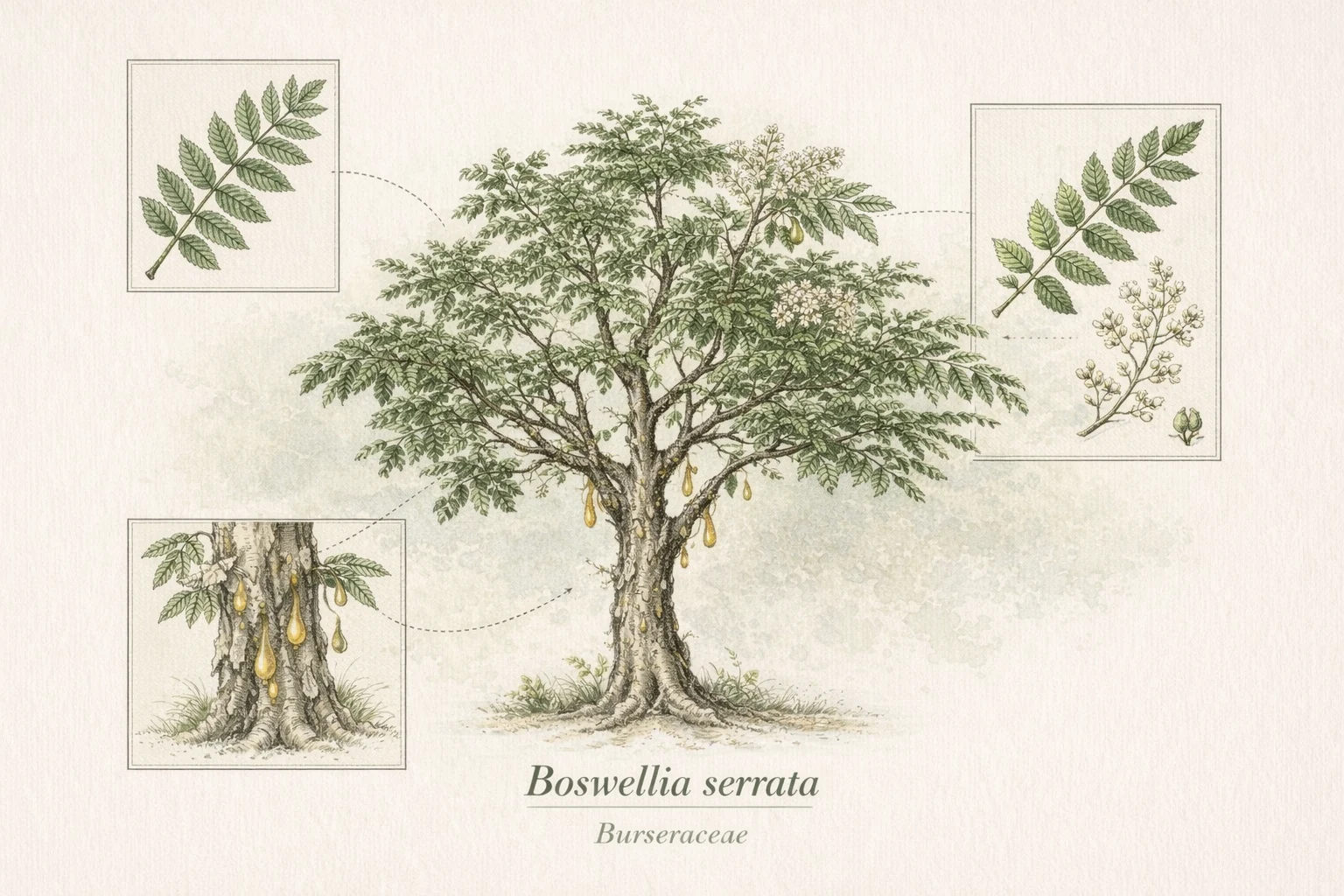
Boswellia serrata · Burseraceae